Blood Lipid Changes With A Well-Formulated Ketogenic Diet In Context






Understanding the Total Risk ‘Forest’ Rather than Focusing on the ‘LDL Tree’
For the last 5 decades, most medical and nutrition scientists have focused on low density lipoprotein (LDL) cholesterol as a primary cause of coronary heart disease. Characterized as ‘bad cholesterol,’ literally thousands of studies have been done using drugs or diet to reduce LDL cholesterol and thereby hoping to reduce heart attacks and mortality. While cholesterol lowering therapy has become the standard of care for some individuals with well-defined heart disease risk, this focus on cholesterol in general—and LDL cholesterol in particular—remains very controversial.
Part of this controversy stems from our tendency as scientists to reduce a problem to its simplest component(s). Unfortunately the standard measure of blood LDL cholesterol is easy but inaccurate (Volek Phinney 2011), and even when the various components of the blood LDL are accurately measured (Reaven 1993) they represent only a fraction of the lipid and other biomarkers of heart disease risk. In other words, in the interest of ‘keeping it simple,’ we have wrongly ignored the rest of the ‘forest’ of other risk factors while focusing on the LDL cholesterol ‘tree.’
A turning point in understanding the limitations of LDL and heart disease came with the publication of the Lyon Diet Heart Study (de Lorgeril 1994, 1999). This randomized trial pitted a standard low fat diet against a Mediterranean diet for people with a prior heart attack. The study was halted after 2.7 years because there was a dramatic reduction in repeat heart attack incidence and overall mortality in the Mediterranean diet group. But to everyone’s astonishment, there was no difference in LDL cholesterol changes between the Mediterranean and low fat diet groups. At least for this diet study, the standard calculated LDL value did not seem to matter that much. Nor did most of the other standard biomarkers of that era that they measured, indicating that some very important drivers of coronary disease risk were going unmeasured. In the intervening 20 years, however, the range of factors linked to heart attack risk has expanded greatlyi.e., the forest has gotten a lot bigger.
In our recently published 1-year results from the IUH/Virta diabetes reversal study, we reported a small but significant rise in the average blood LDL cholesterol level in our patients on a well-formulated ketogenic diet (Hallberg, 2018). At the same time, however, we noted major reductions in a number of coronary disease risk factors including weight, blood pressure, and of course HbA1c. But now we have published a much more extensive review of these risk factor changes for this group of about 200 patients after a year of Virta Treatment (Bhanpuri 2018). As a snap-shot of this ‘tree view’ versus a ‘forest view,’ here are two contrasting figures that demonstrate just how complex this picture is, but also the pattern of how these other risk factors change independent of the variable changes in LDL.
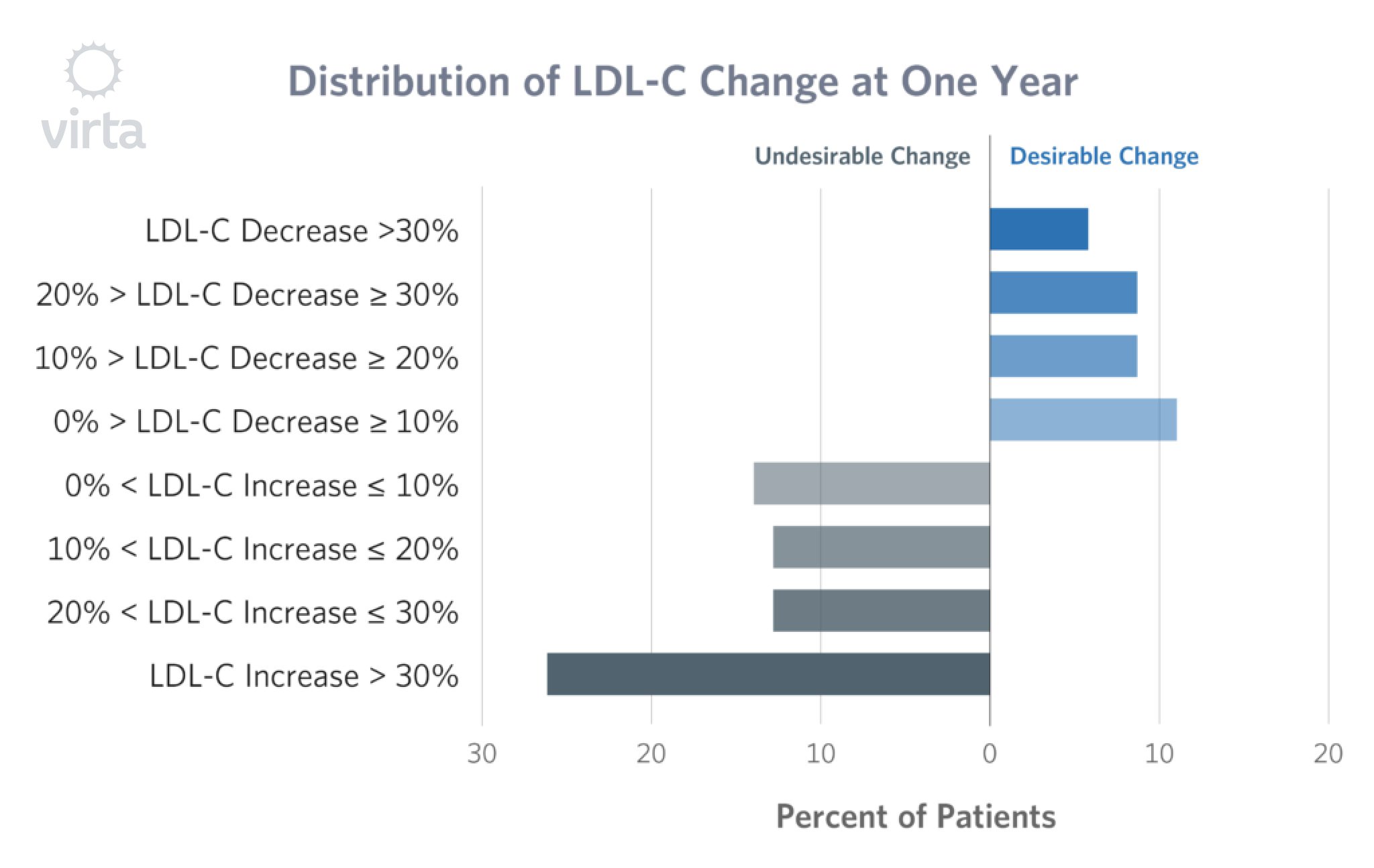
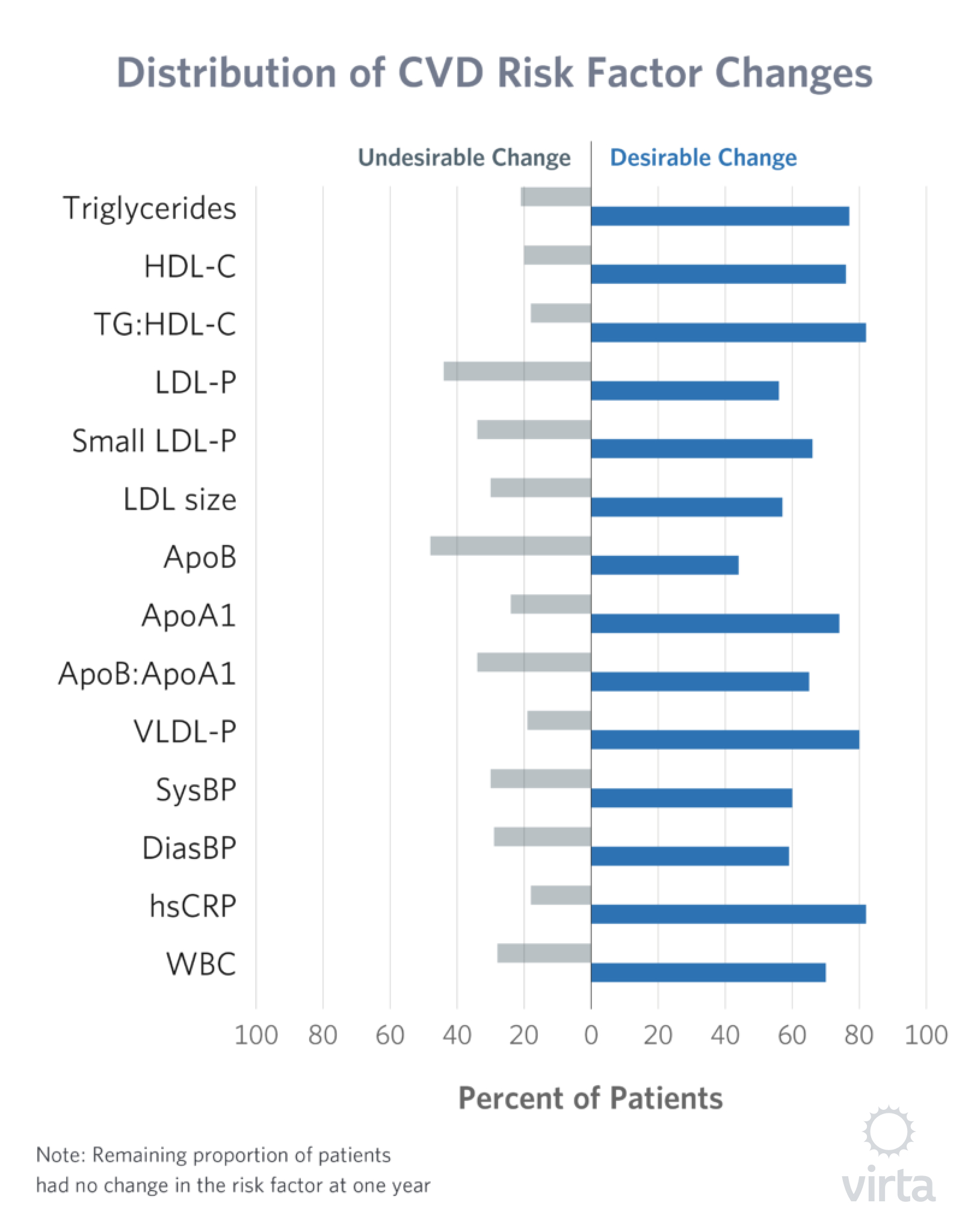
In Figure 1, one can see that the number of patients whose LDL went up was somewhat greater than the number whose LDL went down. In the Figure 2, 14 other risk factor are depicted in the same manner where numbers with improved risk far outweigh those indicating a negative response. From this perspective, the heart disease risk ‘forest’ indicates that a well-formulated ketogenic diet is much healthier than one might conclude by focusing on the single LDL ‘tree.’
Novel results from the IUH Diabetes Reversal Study
Here is a table with the actual numbers for each of the risk factors shown in the figures above, plus HbA1c and weight. For each factor, we show the change between baseline and 1-year as a percent, the P-value indicating the chance this change might occur at random (i.e., the smaller the better), and then arrows up or down indicating how this change might influence overall heart disease and mortality risk.
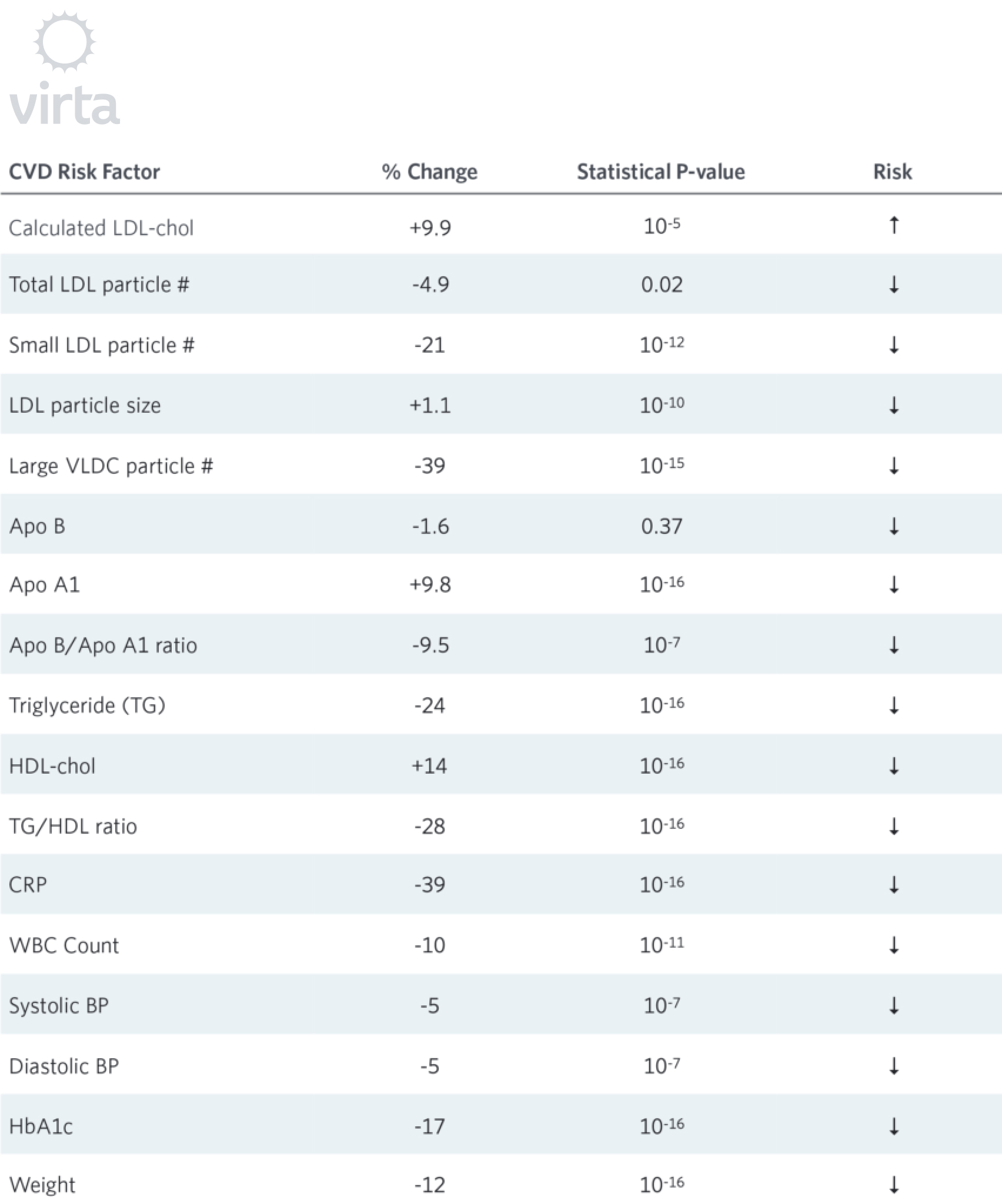
So why are these results novel? Two reasons. While short term studies of ketogenic diets given to patients with type 2 diabetes lasting a few weeks (Boden 2005) to a few months (Snel 2009, Lean 2017) have demonstrated dramatic improvements in HbA1c and glycemic control, none have sustained these benefits without weight regain and/or rising HbA1c values after 1 year. Second, no prior prospective outpatient low carbohydrate diet study has documented any thing near this degree (0.6 mM at 10 weeks and 0.3 to 0.4 mM at one year) of sustained nutritional ketosis in such a large cohort past the first few months of treatment. Note that only the arrow for calculated LDL cholesterol points up, whereas all of the other 16 point down. It is also worthy of note that of these 16, only two have associated P-values that are non-significant or borderline. All of the others indicate that the chance of random error is less than 10-5 (which translates to less than 1-in-ten-thousand). What this means in turn is that these observations of reduced risk are statistically very robust.
This sustained nutritional ketosis may be a pivotal factor in the broad-spectrum of risk reductions associated with the Virta Treatment. Long thought to be a secondary metabolite of fat oxidation by the liver, beta-hydroxybutyrate (BOHB) is now understood to be a potent epigenetic signal controlling the body’s defenses against oxidative stress (Shimazu 2013), inflammation (Youm 2014), and insulin resistance (Newman 2015). Taken together, this combination of pharmaceutical-potency effects of BOHB can explain why the Virta Treatment is a novel intervention that can deliver robust and sustained benefits.
What Blood Lipids Actually Do
When we think of various tests as risk factors, we sometime tend to forget what those substances actually do in the body and why their levels change (or not) when we change our diet. For example, we have known for a long time that blood levels of both cholesterol and saturated fat tend to be independent of how much of these nutrients we eat. (Volek Phinney, The Sad Saga of Saturated Fat; Volek Phinney, You Are Not What You Eat). For other essential nutrients like omega-3 fats, blood and tissue levels tend to be quite responsive to dietary intakes.
But a completely different set of factors come into play when we eat less energy than we burn, which forces the body to dip into its energy stores and thus mobilize body fat. Similarly, when we restrict dietary carbohydrates, either body fat or dietary fat has to become the body’s principle source of energy. This is most profound in the keto-adapted state, where circulating lipids and blood ketones (made from fat in the liver) together provide 75-85% of the body’s energy. In other words, eating more fat requires that more of it pass through the bloodstream. Lipoproteins play a critical role in the transport of lipid in the bloodstream, so changes in delivery needs in turn will impact lipoprotein lab results.
In reality, the changes in how the body processes, transports, and uses fat for energy after becoming keto-adapted are very complex. In response to the state of nutritional ketosis, humans can more than double their rates of fat oxidation (i.e., use for fuel) at rest and during exercise (Phinney 1983, Volek Phinney 2012, Volek 2016). So when you combine a doubling of fat intake with a doubling of fat use, clearly a lot more fat has to pass through the bloodstream. And the mysteries here are how and why this can be safely accomplished, and how these dramatic changes in fat transport are reflected in a standard fasting blood lipid panel.We have spent a few decades studying how the body adapts to a well-formulated ketogenic diet, and have come to recognize a pretty consistent pattern for the changes in most blood lipids, but a quite inconsistent pattern for the calculated LDL cholesterol level in particular. The consistent changes are:
- a dramatic reduction in serum triglycerides
- a rise in HDL cholesterol
- and the same or lower levels of saturated fats in serum triglycerides
As noted above, the one inconsistent variable in this otherwise predictable pattern of change is the calculated serum LDL cholesterol level. For some people, following a ketogenic diet makes their LDL cholesterol go down and for some it does not change. But for a fair number of people the calculated LDL cholesterol value rises, in some cases quite a lot. Thus the key question from this topic is: How important is the calculated LDL cholesterol relative to the other risk factors that have been recently characterized?
Why LDL Cholesterol is Not a Single Number
There are two important limitations of the commonly reported serum LDL cholesterol level. First, the usual test procedure does not actually measure LDL – it reports a calculated value based upon measurements of serum total and HDL cholesterol and triglycerides, along with a number of assumptions. And in particular, when the triglyceride value undergoes a big change, it can skew the calculated LDL value considerably (Volek Phinney 2011). Second, the circulating lipoprotein particles classed as LDL are actually quite diverse in size, and it is now recognized that the smaller, more dense particles (which carry proportionately less triglyceride) are the sub-fraction that is associated with vascular damage and heart disease (Austin 1988, Berneis 2002).
As noted in our recent study data, all but one of the biomarkers of cardiovascular risk that we measured moved in a beneficial direction, and for most of these the changes were statistically significant. Only the calculated LDL cholesterol value went in the ‘wrong direction.’ But in this case, it appears that this was due to a shift to a greater proportion of the larger particles because the total particle number did not change, the average particle size increased, while the small dense particle number was significantly decreased.
Inflammation as an Independent Risk Factor for Coronary Vascular Disease
The idea that there are other important CVD risk factors beside cholesterol and its distribution among lipoproteins is not new. Starting over three decades ago, a number of mainstream investigators have noted that the total white blood cell count (Yarnell 1985, Kannel, 1992) and then c-reactive protein (Ridker 1996) levels appear to predict coronary disease and mortality independent of cholesterol.
The key question as to whether this was a mere association or causal has been addressed by two major studies. The JUPITER study assessed the response of patients with high CRP but non-elevated LDL cholesterol levels to the anti-inflammatory effects of a statin drug (Ridker 2008). Coronary events were significantly reduced within 2 years, but the effects of the statin on inflammation compared to further reductions in LDL cholesterol could not be definitively separated. This question was resolved with the recent CANTOS Trial (Ridker 2017), in which a mono-clonal antibody against IL-1 beta reduced coronary risk by 15% without any effect on LDL cholesterol levels.
Unfortunately a side effect of of the antibody used in this study (an increase in fatal infections) cancelled out the coronary disease risk reduction, so the CANTOS Trial answered an important question but did not offer an therapeutic solution. However this does offer an interesting insight into the mystery of why the Lyon Diet Heart Study reduced coronary disease risk AND mortality. In that study, blood anti-oxidant levels increased and granulocytes (aka white blood cells) decreased, suggesting that a dietary anti-inflammatory intervention can have potent benefits absent the dangerous side-effects of anti-inflammatory drugs.
Seen from this perspective, the statistically robust anti-inflammatory effects observed in our current study highlight a demonstrably important portion of the coronary disease ‘risk forest’ that is independent of cholesterol.
Blood Saturated Fats and CVD Risk
The levels of saturated fats in various blood lipid fractions—and particularly the 16-carbon saturated fat called palmitate—have long been known to be correlated with risk for heart disease, type 2 diabetes, and mortality (Wang 2003). We have previously posted a detailed review of this topic in our blog The Sad Saga of Saturated Fat. The key fact to keep in mind is that while a primary source of saturated fat in the blood is de novo lipogenesis (i.e., the production of fat from excess dietary carbohydrate) (Aarsland 2003), there is little if any relationship between dietary saturated fat intake and blood saturated fat content. And most importantly, because the keto-adapted state doubles the body’s ability to burn saturated fat for fuel while at the same time shutting down de novo lipogenesis, blood levels of saturated fats are reduced independent of dietary saturated fat intake (Forsythe 2008 & 2010, Volk 2014). Thus we have another disconnect between dogma and data: a risk factor that goes down with a well-formulated ketogenic diet despite the ‘diet-heart disease hypothesis’ which tries to link dietary saturated fat to blood cholesterol levels.
Getting Beyond Single Biomarkers of Cardiovascular Risk
Given the host of biomarkers reflecting a wide range of processes that contribute to atherosclerosis and coronary artery disease risk, the recognition that we need a multifactorial equation that encompasses this heterogeneous process rather than striving for a single reductionist approach is finally gaining traction (Yeboah 2016). Based upon published 2013 guidelines, the American College of Cardiology now offers a 10-year heart disease risk predictor that includes the following inputs:
- age
- sex
- race
- total cholesterol
- HDL cholesterol
- LDL cholesterol
- systolic blood pressure
- diastolic blood pressure
- diabetes
- smoking
- medication use: statin, hypertension, aspirin
Based upon this equation, the 10-year atherosclerotic cardiovascular disease (ASCVD) risk score in our recent study decreased -11.9% (P = 5×10⁻⁵). This is a large beneficial effect experienced by the participants in our study despite the observed changes in calculated LDL values. And this equation does not take into account improvements in inflammation and saturated fats that would reduce this risk prediction even further.
Summary
Biomarkers of cardiovascular disease risk represent our scientific attempt to find a crystal ball that predicts future disease and guides rational therapeutic intervention. In a case where so many different factors are associated with coronary risk, we need to avoid the reductionist temptation to focus on a single tree over the contribution of the entire forest.
Ideally, in the future we will have results on CVD and mortality risk from a large randomized controlled trial pitting a well-formulated ketogenic diet against the best that usual care can offer. In the interim, we have demonstrated that a continuous care treatment including nutritional ketosis in patients with type 2 diabetes improved most biomarkers of CVD risk after one year. The increase in LDL-cholesterol appeared limited to the large LDL sub-fraction; whereas LDL particle size increased, total LDL-P and ApoB were unchanged, and inflammation and blood pressure decreased.
Dr. Sarah Hallberg on How Virta Improves Cardiovascular Risk Factors
The information we provide at virtahealth.com and blog.virtahealth.com is not medical advice, nor is it intended to replace a consultation with a medical professional. Please inform your physician of any changes you make to your diet or lifestyle and discuss these changes with them. If you have questions or concerns about any medical conditions you may have, please contact your physician.
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

- Aarsland A, Wolfe RR. Hepatic secretion of VLDL fatty acids during stimulated lipogenesis in men. J Lipid Res. 1998; 39:1280-6.
- Austin MA, Breslow JL, Hennekens CH, Buring JE, Willett WC, Krauss RM. Low-Density Lipoprotein Subclass Patterns and Risk of Myocardial Infarction. JAMA. 1988; 260:1917-1921. doi:10.1001/jama.1988.03410130125037
- Berneis KK, Krauss RM. Metabolic origins and clinical significance of LDL heterogeneity. J Lipid Res. 2002; 43:1363-1379. doi: 10.1194/jlr.R200004-JLR200
- Bhanpuri NH, Hallberg SJ, Williams PT, et al. Cardiovascular Disease Risk Factor Responses to a Type 2 Diabetes Care Model Including Nutritional Ketosis Induced by Sustained Carbohydrate Restriction at One Year: An Open Label, Non-Randomized, Controlled Study. Cardiovascular Diabetology. 2018; 17:56, https://doi.org/10.1186/s12933-018-0698-8.
- Boden G, Sargrad K, Homko C, Mozzoli M, Stein TP. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Ann Intern Med. 2005;142:403–11.
- Forsythe CE, Phinney SD, Fernandez ML, Quann EE, Wood RJ, Bibus DM, Kraemer WJ, Feinman RD, Volek JS. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids. 2008; 43:65-77.
- Forsythe CE, Phinney SD, Feinman RD, et al. Limited effect of dietary saturated fat on plasma saturated fat in the context of a low carbohydrate diet. Lipids. 2010; 45:947-62. doi: 10.1007/s11745-010-3467-3.
- de Lorgeril M, Renaud S, Salan P, et al. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. The Lancet. 1994; 343:1454-1459.
- de Lorgeril M, Salen P, Martin JL, et al. Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications After Myocardial Infarction. Final Report of the Lyon Diet Heart Study. Circulation. 1999; 99:779-785.
- Kannel WB1, Anderson K, Wilson PW. White blood cell count and cardiovascular disease. Insights from the Framingham Study. JAMA. 1992; 267:1253-6.
- Lean MEJ, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. The Lancet. 2018; 391 513-630.
- Newman JC, Verdin E. β-hydroxybutyrate: much more than a metabolite. Diabetes Res Clin Pract. 2014; 106:173-81. doi: 10.1016/j.diabres.2014.08.009.
- Phinney SD, Bistrian BR, Evans WJ, Gervino E, Blackburn GL. The human metabolic response to chronic ketosis without caloric restriction: preservation of submaximal exercise capability with reduced carbohydrate oxidation. Metabolism. 1983; 32:769-76.
- Reaven GM, Ida Chen Y-D, Jeppesen J, Maheux P, Krauss RM. Insulin reistance and hyperinsulinemia in individuals with small, dense low density lipoprotein particles. J Clin Invest. 1993; 92:141-146.
- Ridker PM, Buring JE, Shih J, Matias M, Hennekens CH. Prospective study of C-reactive protein and the risk of future cardiovascular events among apparently healthy women. Circulation. 1998; 98:731-3.
- Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008 Nov 20;359(21):2195-207.
- Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017; 377:1119-1131.
- Shimazu T, Hirschey MD, Newman J, et al. Suppression of oxidative stress by β-hydroxybutyrate, an endogenous histone deacetylase inhibitor. Science. 2013; 339:211-4. doi: 10.1126/science.1227166.
- Snel M. The Effects of a Very Low Calorie Diet and Exercise in Obese Type 2 Diabetes Mellitus Patients. © 2011, Marieke Snel, Leiden, The Netherlands. ISBN: 978-94-6169-102-6
- Volek JS, Freidenreich DJ, Saenz C, et al. Metabolic characteristics of keto-adapted ultra-endurance runners. M Metabolism. 2016; 65:100-10.
- Volek J, Phinney S. The Art and Science Of Low Carbohydrate Living. 2011. Beyond Obesity LLC, Miami, FL
- Volek J, Phinney S. The Art and Science Of Low Carbohydrate Performance. 2012. Beyond Obesity LLC, Miami, FL
- Volek J, Phinney S. The Sad Saga of Saturated Fat. Virta Blog Post
- Volek J, Phinney S. You Are Not What You Eat. http://www.artandscienceoflowcarb.com/you-are-not-what-you-eat/
- Volk BM, Kunces LJ, Freidenreich DJ, et al. Effects of step-wise increases in dietary carbohydrate on circulating saturated Fatty acids and palmitoleic Acid in adults with metabolic syndrome. PLoS One. 2014; 9:e113605. doi: 10.1371/journal.pone.0113605.
- Wang L, Folsom AR, Eckfeldt JH. Plasma fatty acid composition and incidence of coronary heart disease in middle aged adults: the Atherosclerosis Risk in Communities (ARIC) Study. Nutr Metab Cardiovasc Dis. 2003; 13:256-66.
- Yarnell JW, Sweetnam PM, Elwood PC, et al. Haemostatic factors and ischaemic heart disease. The Caerphilly study. Br Heart J. 1985; 53:483-7.
- Yeboah J, Young R, McClelland RL, et al. Utility of Nontraditional Risk Markers in Atherosclerotic Cardiovascular Disease Risk Assessment. J Am Col Cardiology. 2016; 67:139-147.
- Youm YH, Nguyen KY, Grant RW, et al. The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome-mediated inflammatory disease. Nat Med. 2015; 21:263-9. doi:10.1038/nm.3804.